
Table of Contents >> Show >> Hide
- What a Lumbar MRI Actually Shows
- How to Read a Lumbar MRI Report Step by Step
- What Normal Lumbar MRI Results May Look Like
- Common Abnormal Lumbar MRI Findings Explained
- How to Tell Whether an Abnormal Finding Matters
- Red Flags: When Lumbar MRI Findings or Symptoms Need Urgent Care
- Specific Examples of Lumbar MRI Report Language
- Questions to Ask Your Doctor After a Lumbar MRI
- Practical Experience: What People Often Learn After Reading Their Lumbar MRI
- Conclusion
Opening a lumbar MRI report can feel like reading a weather forecast written by a robot with a medical degree: “mild desiccation,” “broad-based protrusion,” “foraminal narrowing,” and suddenly your lower back sounds like a construction site. The good news is that lumbar MRI results are not impossible to understand. With a few basic landmarks and some plain-English translation, you can learn how to read the report, recognize what looks normal, understand common abnormal findings, and know which phrases deserve a calm conversation with your doctornot a midnight internet panic spiral.
A lumbar MRI is a detailed scan of the lower spine. It shows the vertebrae, discs, spinal canal, nerve roots, joints, ligaments, bone marrow, and nearby soft tissues. Doctors use it to evaluate back pain, sciatica, numbness, weakness, trauma, infection, tumors, spinal stenosis, disc herniation, and symptoms that may suggest nerve compression. MRI is especially useful because it shows soft tissues better than a standard X-ray.
Medical note: This guide is educational and is not a diagnosis. MRI findings must be interpreted with symptoms, physical examination, medical history, and the radiologist’s official report. Many people have disc bulges or degenerative changes on MRI without pain, so the scan is only one piece of the puzzle.
What a Lumbar MRI Actually Shows
The lumbar spine usually includes five vertebrae labeled L1 through L5. Below L5 is the sacrum, so the bottom level is often written as L5-S1. Between each vertebra sits an intervertebral disc, which acts like a cushion. Behind the vertebral bodies is the spinal canal, where nerve structures travel. At each level, nerve roots exit through small openings called foramina.
Most lumbar MRI reports are organized by spinal level: L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1. That format helps the radiologist describe whether each level looks normal or shows changes such as disc degeneration, bulging, herniation, stenosis, arthritis, or nerve compression.
Common MRI Views and Sequences
MRI images are taken in different directions. Sagittal images are side views, like slicing a loaf of bread from front to back. Axial images are cross-sectional views, like looking down at a single spinal level from above. Radiologists also use different MRI sequences. T1-weighted images are helpful for anatomy and bone marrow. T2-weighted images make fluid appear bright, which helps show discs, nerves, inflammation, and spinal fluid. You do not need to become a radiologist, but knowing these basics makes the report less mysterious.
How to Read a Lumbar MRI Report Step by Step
1. Start With the Indication
The indication explains why the MRI was ordered. It may say “low back pain,” “right-sided sciatica,” “leg weakness,” “history of surgery,” or “rule out stenosis.” This matters because the most important MRI finding is the one that matches the patient’s symptoms. A tiny left-sided disc bulge may not explain severe right-sided leg pain. In other words, the MRI should match the story your body is telling.
2. Check the Technique and Contrast
The technique section describes how the scan was performed. Most lumbar MRIs are done without contrast. Contrast dye may be used when doctors need to evaluate infection, tumors, inflammation, scar tissue after surgery, or certain complex conditions. If the report says “without IV contrast,” that is very common and not automatically a problem.
3. Look at Alignment
Alignment tells whether the bones are stacked normally. A normal report may say “normal lumbar lordosis” or “no spondylolisthesis.” Lumbar lordosis is the natural inward curve of the lower back. Abnormal alignment may include spondylolisthesis, where one vertebra slips forward or backward compared with the one below it. Mild slips can be stable and managed conservatively, but larger or symptomatic slips may need specialist evaluation.
4. Review Vertebral Bodies and Bone Marrow
The vertebral bodies are the main block-like bones of the spine. A normal MRI may say vertebral body heights are maintained and marrow signal is normal. Abnormal findings may include compression fractures, bone bruising, suspicious marrow lesions, infection, or inflammatory changes. Words like “acute fracture,” “mass,” “discitis,” “osteomyelitis,” or “metastatic disease” are more serious and should be discussed promptly with a clinician.
5. Evaluate the Discs
Discs are one of the main stars of a lumbar MRI report. Normal discs usually have good height and hydration. On T2 images, a healthy disc often appears brighter because it contains more water. With aging or wear, discs can lose water, flatten, darken, bulge, or herniate. This process is often called disc desiccation or degenerative disc disease. Despite the dramatic name, degenerative disc disease is usually a description of wear-and-tear changes, not a single disease attacking your spine with tiny villain gloves.
6. Read the Canal, Lateral Recesses, and Foramina
The spinal canal is the central passageway. The lateral recesses are side zones where nerve roots travel before exiting. The neural foramina are the exit tunnels for nerves. Narrowing in these spaces is called stenosis. Stenosis may be mild, moderate, or severe. The key question is whether narrowing compresses or irritates a nerve root in a way that matches symptoms such as sciatica, numbness, tingling, or weakness.
7. Do Not Skip the Impression
The impression is the summary at the end of the report. If you only read one section, read this one first. It usually lists the most important findings in priority order. The body of the report gives details, but the impression tells you what the radiologist thinks matters most.
What Normal Lumbar MRI Results May Look Like
A normal lumbar MRI report may include phrases such as:
- Normal lumbar alignment.
- Vertebral body heights are maintained.
- No acute fracture or suspicious marrow lesion.
- Conus medullaris terminates normally.
- No significant disc bulge or herniation.
- No central canal stenosis.
- No neural foraminal narrowing.
- No nerve root compression.
The conus medullaris is the lower end of the spinal cord, usually ending around L1-L2. Below that, the nerve roots continue downward as the cauda equina. A normal report may say the conus is normal in position and signal. That is reassuring.
However, “normal” does not always mean pain-free, and “abnormal” does not always mean dangerous. Muscle strain, ligament irritation, sacroiliac joint issues, hip problems, inflammatory conditions, and nerve sensitivity may cause pain even when the lumbar MRI looks clean. Meanwhile, mild disc bulges can appear on scans of people who feel perfectly fine.
Common Abnormal Lumbar MRI Findings Explained
Disc Desiccation
Disc desiccation means the disc has lost some water content. It often appears darker on T2 MRI images. This is common with aging and may or may not cause symptoms. If the report says “mild disc desiccation at L4-L5 and L5-S1,” it usually means early degenerative change. Think of it as a disc looking a little less like a fresh grape and a little more like a raisinnot ideal, but not automatically catastrophic.
Disc Bulge
A disc bulge means the outer edge of the disc extends beyond its usual boundary over a broad area. Bulges are common and often age-related. A report may say “mild diffuse disc bulge without significant stenosis.” That usually means the disc is slightly expanded but not clearly pressing on nerves.
Disc Protrusion, Extrusion, and Sequestration
A disc protrusion is a more focal herniation where disc material pushes outward. A disc extrusion means disc material has pushed farther out through the outer disc layer. Sequestration means a fragment has separated from the main disc. These findings can matter more when they contact or compress a nerve root.
Example: “Right paracentral disc extrusion at L5-S1 impinging the right S1 nerve root.” In plain English, a piece of disc is sticking out toward the right side at the bottom lumbar level and pressing on the nerve that can cause pain down the back of the leg. That finding may match classic sciatica.
Annular Fissure
An annular fissure is a tear in the outer ring of the disc. Some reports call it an “annular tear.” It can be associated with back pain, but it can also be found incidentally. The seriousness depends on symptoms, inflammation, and whether there is associated herniation or nerve irritation.
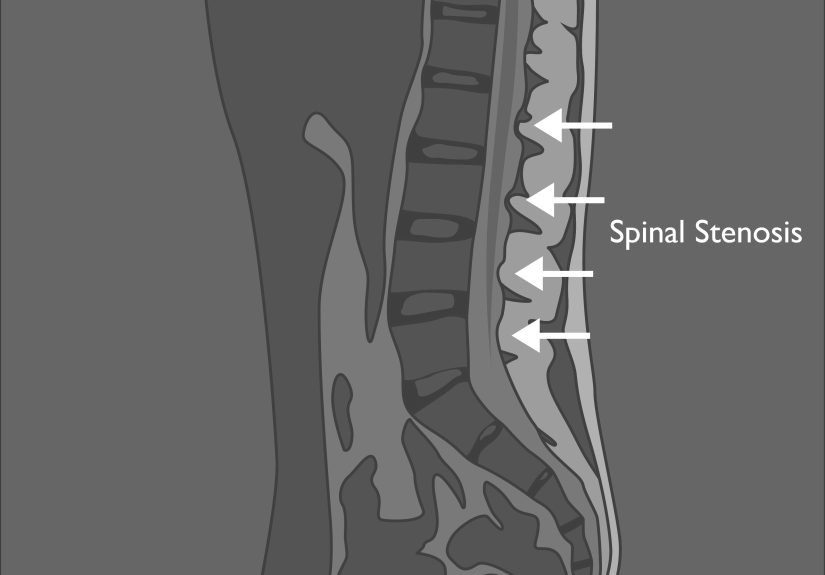
Spinal Stenosis
Spinal stenosis means narrowing of the spinal canal or nerve passageways. Central canal stenosis occurs in the main canal. Lateral recess stenosis affects the side channel where nerve roots travel. Foraminal stenosis affects the exit opening where a nerve leaves the spine.
Mild stenosis may not cause symptoms. Moderate or severe stenosis can cause leg pain, numbness, heaviness, cramping, or weakness, especially while walking or standing. Many people with lumbar spinal stenosis feel better when sitting or leaning forward, which opens the canal slightly. This is why some people with stenosis love shopping cartsnot for the groceries, but for the forward-leaning posture.
Facet Arthropathy
Facet joints are small joints at the back of the spine. Facet arthropathy means arthritis or degenerative change in these joints. It may contribute to back stiffness, pain with extension, or stenosis if enlarged joints narrow nerve spaces. Reports may describe “mild,” “moderate,” or “severe” facet arthropathy.
Ligamentum Flavum Thickening
The ligamentum flavum is a ligament inside the spinal canal. It can thicken with age and contribute to stenosis. When combined with disc bulging and facet arthritis, it can reduce space around nerves. A report might say “disc bulge, facet arthropathy, and ligamentum flavum hypertrophy resulting in moderate central canal stenosis.” Translation: several wear-and-tear changes are teaming up to crowd the canal.
Spondylolisthesis
Spondylolisthesis is slippage of one vertebra over another. It is often graded by severity. Grade 1 is mild. It may occur from arthritis, congenital defects, stress fractures, or trauma. Symptoms depend on instability and nerve compression. Some people have it for years with minimal symptoms; others develop back pain or leg symptoms.
Modic Changes and Endplate Changes
Endplates are the surfaces where discs meet vertebral bodies. Modic changes describe MRI signal changes in the bone marrow near the endplates. They are often associated with degeneration. Some types may reflect inflammation or fatty change. These findings are not rare and should be interpreted in context.
Compression Fracture
A compression fracture means a vertebral body has partially collapsed. MRI can help determine whether a fracture is recent or old by showing bone marrow swelling. New fractures may cause sudden severe pain, especially after trauma or in people with osteoporosis.
Infection, Tumor, or Inflammatory Disease
Less common but important abnormal findings include spinal infection, tumor, inflammatory arthritis, abscess, or suspicious marrow replacement. Words such as “enhancing mass,” “epidural abscess,” “discitis,” “osteomyelitis,” or “malignancy” require direct medical follow-up. These are not findings to decode casually between coffee and email.
How to Tell Whether an Abnormal Finding Matters
The most important rule is simple: match the MRI finding to the symptoms. A left L5-S1 disc herniation pressing the left S1 nerve root may explain left-sided sciatica traveling down the back of the thigh and calf. But it may not explain right-sided groin pain. A small disc bulge with no stenosis may sound scary but may not be clinically significant.
Severity words also matter. “Mild” usually means small or early change. “Moderate” means more noticeable narrowing or degeneration. “Severe” suggests significant narrowing, compression, or structural change. Still, even severe-sounding imaging must be interpreted by a qualified clinician. Some people have impressive MRI findings and modest symptoms; others have terrible pain with subtle imaging findings.
Red Flags: When Lumbar MRI Findings or Symptoms Need Urgent Care
Seek urgent medical attention if back pain is associated with new bladder or bowel dysfunction, numbness in the saddle area, rapidly worsening leg weakness, fever with severe back pain, recent major trauma, history of cancer with new unexplained back pain, unexplained weight loss, or signs of infection. These symptoms may suggest serious conditions such as cauda equina syndrome, fracture, infection, or tumor.
Cauda equina syndrome is rare but serious. It involves compression of the nerve roots at the lower end of the spinal canal and can cause bladder problems, bowel problems, saddle numbness, severe leg weakness, or major neurologic changes. This is an emergency, not a “let’s see how it feels after the weekend” situation.
Specific Examples of Lumbar MRI Report Language
Example 1: Mild Degenerative Change
Report phrase: “Mild disc desiccation and shallow broad-based disc bulge at L4-L5 without significant canal or foraminal stenosis.”
Plain English: The disc at L4-L5 shows mild wear and a small bulge, but it is not significantly narrowing nerve spaces. This may be an age-related finding and may not be the main pain source.
Example 2: Nerve Root Compression
Report phrase: “Left paracentral disc protrusion at L5-S1 contacts the descending left S1 nerve root.”
Plain English: A disc herniation near the bottom of the lumbar spine is touching the left S1 nerve. If the patient has left-sided sciatica, this could be clinically meaningful.
Example 3: Spinal Stenosis
Report phrase: “Moderate central canal stenosis at L4-L5 due to disc bulge, facet arthropathy, and ligamentum flavum hypertrophy.”
Plain English: Several degenerative changes are narrowing the main spinal canal at L4-L5. This may cause leg symptoms, especially with walking or standing.
Example 4: Foraminal Narrowing
Report phrase: “Severe right neural foraminal stenosis at L5-S1 with compression of the exiting right L5 nerve root.”
Plain English: The exit tunnel for the right L5 nerve is very narrow, and the nerve appears compressed. If symptoms travel down the right leg in an L5 pattern, this finding may be important.
Questions to Ask Your Doctor After a Lumbar MRI
- Which MRI finding best matches my symptoms?
- Is there nerve compression, or only age-related change?
- Is the narrowing mild, moderate, or severe?
- Do I need physical therapy, medication, injections, or a surgical opinion?
- Are there any urgent findings?
- How does this MRI compare with any older imaging?
- What symptoms should make me seek urgent care?
Practical Experience: What People Often Learn After Reading Their Lumbar MRI
One of the most common real-world experiences with lumbar MRI results is emotional whiplash. A person goes into the scan hoping for answers, then receives a report full of alarming words. “Degeneration” sounds like the spine is crumbling. “Bulge” sounds like something is about to burst. “Stenosis” sounds like a door has slammed shut inside the back. But after a careful review with a clinician, many patients learn that some findings are common and manageable.
A helpful approach is to read the report in layers. First, look at the impression. This is the radiologist’s highlight reel. Second, identify the level involved. L4-L5 and L5-S1 are common troublemakers because they carry a lot of mechanical stress. Third, look for words that describe nerve involvement: “contacts,” “displaces,” “impinges,” “compresses,” or “no nerve root compression.” These words matter more than the mere presence of a bulge.
Another useful lesson is that symptoms are the compass. If the MRI shows right L5 nerve compression and the person has pain running down the right outer leg into the top of the foot, the imaging and symptoms may line up. If the MRI shows mild left-sided narrowing but symptoms are mostly central back stiffness after sitting, the finding may be less important. This is why doctors examine strength, reflexes, sensation, walking pattern, and pain distribution instead of treating the MRI like a magic fortune cookie.
Patients also often discover that “abnormal” does not always mean “surgery.” Many lumbar MRI findings are treated first with conservative care: activity modification, physical therapy, anti-inflammatory medication when appropriate, posture and movement changes, weight management, injections, or time. Surgery may be considered when there is severe nerve compression, progressive weakness, disabling symptoms that do not improve, or emergency conditions. But a disc bulge alone is not a golden ticket to the operating room.
It also helps to bring the report to an appointment with specific notes. Write down where the pain travels, what makes it worse, what makes it better, whether there is numbness or weakness, and how long symptoms have been present. Mention whether walking, standing, bending forward, coughing, or sitting changes the pain. These details help the doctor connect the scan to the real-life problem.
Finally, avoid comparing your MRI to someone else’s. Two people can have nearly identical reports and completely different symptoms. Your spine is not a competition, and there is no trophy for “most dramatic L5-S1.” The goal is not to collect scary terms; the goal is to understand what matters, ignore what does not, and build a treatment plan that helps you move, sleep, work, and live better.
Conclusion
Learning how to read and recognize normal and abnormal lumbar MRI results can make the report far less intimidating. A normal MRI usually shows good alignment, maintained vertebral height, healthy nerve spaces, and no significant disc herniation or stenosis. Abnormal findings may include disc desiccation, bulges, herniations, stenosis, facet arthritis, ligament thickening, spondylolisthesis, fractures, infection, or tumors. The key is not simply spotting abnormalities; it is understanding whether they match the symptoms and whether they require routine care, specialist evaluation, or urgent attention.
The smartest way to read a lumbar MRI is with curiosity, not panic. Start with the impression, learn the spinal levels, translate the major terms, and ask your healthcare provider which findings actually matter for your body. Your MRI is a map, not a verdict.





